Location: Home >> Detail
J Sustain Res. 2024;6(2):e240011. https://doi.org/10.20900/jsr20240011

Faculty of Humanities and Social Sciences, Iwate University, 3-18-34 Ueda, Morioka 020-8550, Japan
National health expenditures are crucial for enhancing citizens’ physical well-being. This study aimed to illustrate the affordability of national medical care services and to identify the medical care system’s role in an aging population. The results indicated that national health expenditures significantly reduce perceived health and income inequalities among countries when removing the aging population effect. Regarding affordability, rising national health expenditures (calculated as a share of the gross domestic product) increase public dissatisfaction with family incomes and decrease satisfaction with medical systems. It showed that improved medical care efficiency and public health among middle-aged and older populations due to various socioeconomic factors are expected to reduce the burden of the aging population.
Good health is essential for individuals’ and families’ well-being. A qualified medical care system or service that offers well-organized, accessible, and affordable healthcare is associated with improved public health [1,2].
Previous studies have theoretically and empirically examined approaches to improving public health by increasing medical care system financing and strengthening service accessibility [3–5]. For example, a study in Africa [6] used a household survey to identify medical care accessibility, availability, and affordability in the context of chronic illnesses. The study concluded that the government should strengthen medical care services to improve access to healthcare and that it should provide financial aid to economically disadvantaged families. In China, the quality of the healthcare system’s quality has improved following reforms in 2000. At that time, health expenditures in the public sector increased rapidly to provide qualified healthcare to rural areas and improve affordability by reducing out-of-pocket payments [3]. Consistent results have indicated that the increase in healthcare system financing lowered the mortality rate during the pandemic [4,5]. Similar to China, universal healthcare in other developing nations in Asia, as well as in Africa and Latin America, has been introduced to reduce out-of-pocket expenditures for impoverished families who cannot afford healthcare [7–9].
Regarding medical care system accessibility, universal healthcare coverage benefits society, reduces health inequality, and improves quality of life. The link between medical care quality offered via accessible, affordable medical care systems or services and health at the individual or family level has been examined in both developed and developing nations [10–20]. Xu et al. [10] argued that the high health expenditures caused by illnesses are significant in some emerging and Latin American countries. The authors highlighted that public healthcare could protect households against the financial crises caused by diseases.
Other studies have considered the influence of demographic changes (e.g., an aging population) on the public evaluation of the medical care system. For example, a study using data derived from 12 Eastern and 16 Western European countries evaluated the cognitive determinants of the health care system, specifically the performance of health care, the public expectations of government healthcare provision, and the medical care system burden due to demographic changes such as aging populations [21]. Using the Bayesian-VAR model, Lopreite et al. [22] found that an aging population positively related increased per capita health expenditures to the GDP per capita in China. Using data derived from Italy, Lopreite and Mauro [23] also investigated the effects of the aging population on national healthcare expenditures. Again, using the Bayesian-VAR model, they determined that there was more response to the aging population.
Furthermore, Choi et al. [24] found that among industrialized countries, individual life expectancy and health-adjusted life expectancy have increased due to better quality healthcare and increased access over the past three decades. However, the number of years of poor health has increased with expanded healthcare access and quality improvement. Osborn et al. [11] investigated the level of satisfaction with the medical care system and the service quality and household affordability of medical systems in 11 developed Western countries. They noted that, unlike adults from other countries, adults in the U.S. experienced specific difficulties affording medical care. However, the Affordable Care Act targeted uninsured American adults, improving healthcare affordability, especially for those in low- and middle-income families [3]. Zhao et al. [25] also found that disruptions to healthcare insurance in prior years were negatively associated with Americans’ affordability of and access to cancer care.
In a study based on the definition of affordability, Glied [26] recommended using exemptions, such as defining appropriate thresholds for U.S. policymakers, to improve affordability. Dubé et al. [27] analyzed how to achieve universal healthcare affordability through economic growth using creative technological innovation to sustain affordable healthcare. They highlighted technological improvements for addressing the aging population’s increasing needs through national health expenditures and enhancing people’s income satisfaction [28]. Bertolazzi et al. [29] observed that older generations’ acceptance of new technology may be associated with a medical care system’s sustainability as new technology achieves cost reduction and satisfies increasing medical service needs among the aging population.
However, even though the healthcare system’s accessibility and affordability for individuals or families have been examined [30], research concerning the relationship between medical care systems and household income satisfaction among the aging population remains scarce. Given that the global population is aging, the affordability of health-related well-being initiatives has attracted growing attention. According to the World Bank, 6.87% of the world’s population was over 65 years old in 2000; the corresponding percentage in 2018 was 8.9%, and this number is continuously increasing [31]. The expenditures of medical care systems or services that ensure public health are also rising. For example, the World Bank calculated that the world’s current health expenditures represented 8.6% of the GDP in 2000 and increased to 10% in 2016. In high-income countries, healthcare-related public expenditures reached 12.53% of the GDP [32]. To establish policy improving public health and preparing for future pandemics, an in-depth understanding of the medical care system and its operating efficiency and the prediction of medical care system regulations for the aging population are crucial [33,34].
This study had three aims. First, the relationship between national health expenditures as a percentage of GDP and the public’s satisfaction with medical care systems and services was investigated, using multinational data to determine self-rated health and income satisfaction. Second, it aimed to establish an association among the percentage of the national population over 65 years of age, national health expenditures as a percentage of GDPs, and individuals’ well-being in terms of health and income satisfaction. Third, it provided a comparison and discussion based on results derived from the above two sets of regression to explore national medical care system affordability and the issue of aging populations.
This study made several contributions to the current literature. First, the results indicated the affordability of national medical care systems because governments subsidize the medical care system with tax revenue. Given the globally aging population, increasing health expenditures is a significant issue for many nations. If public national health expenditures reduce people’s satisfaction with medical care systems and increase the likelihood of household income dissatisfaction, nations may have difficulty providing affordable public medical care systems or services. The results provided insightful implications regarding aging populations for both multinational systems and the general subject of healthcare affordability. To the best of our knowledge, this study is the first to examine the relationship among national health expenditures and the public’s evaluation of medical care system satisfaction, household income satisfaction, and self-rated health, and investigates the effect of the aging population using individual-level data derived from 37 representative countries. The results are expected to provide in-depth insight into establishing long-term health expenditures that consider aging populations.
This paper is organized as follows: Section 2 (METHODS) outlines the data, variables, and empirical modelling strategy that were used; Section 3 (RESULTS AND DISCUSSION) presents the results and discussion; and Section 4 (CONCLUSIONS) concludes the study.
To investigate multinational healthcare, national health expenditures, population aging, and intra-country inequality, we conducted a cross-country, original, and international survey using a web-based version in 32 countries and a face-to-face approach in five countries via a third-party company (Nikkei Research). The third-party company provided reliable, large-volume internet survey data that allowed this study to match the collected data to the population characteristics. The respondents were randomly selected to match the age and gender of the national population. Women older than 60 years were not frequent participants; to match the population’s age and gender, we carefully selected the closest age group. The study design was approved by the appropriate legal and ethics review board of Kyushu University. The data were collected with informed consent was obtained from participants, according to the legal and ethical guidelines. All the methods were in accordance with ethical guidelines and approved by the ethical committee of Kyushu University.
The national health expenditure was presented as a percentage of the GDP, and it was defined as the current health expenditure—which included healthcare goods and services that were consumed in 2016. This health expenditure does not include capital health expenditures (e.g., buildings, machinery, internet technology, and stocks of vaccines for emergencies or outbreaks). Cross-nation health expenditures in this study were collected from the World Bank [22]. Data for the population aged 65 years and older for each country in 2016 were provided by the World Bank [22] and were expressed as a percentage of the total population. Both sets of data are publicly available.
The following countries participated in the survey: Japan, Thailand, Malaysia, Indonesia, Singapore, Vietnam, the Philippines, India, Mongolia, Myanmar, China, Russia, Germany, the United Kingdom, France, Spain, Italy, Sweden, the Netherlands, Greece, Turkey, Hungary, Poland, Czech Republic, Romania, Mexico, Canada, the United States, Venezuela, Chile, Brazil, Colombia, Australia, South Africa, Sri Lanka, and Egypt.
This large-scale survey included 500 to 20,744 observations per country. Other detailed information about the internet survey is provided by Chapman et al. [23]. Specific country-level observation information and the survey start and end times are displayed in Supplementary Table S1.
Variable SettingThe dependent variables to express the participants’ evaluation of medical care systems or services included the following sets of dummy variables: three responses about medical care (important, satisfied, and dissatisfied); two kinds of self-rated health levels (good and poor); and two kinds of income satisfaction (satisfied and dissatisfied). In the survey, the respondents had to indicate whether the medical care system or service was important. For the dummy variables, the important rating was represented as 1, and the other ratings were reported as 0. Similarly, medical care system or service satisfaction ratings were 1 if the respondents were satisfied and 0 for other responses. The medical care system or service dissatisfaction dummy variable was defined as dissatisfied (1) or other (0).
Regarding income satisfaction, participants were instructed to “please select an item that appropriately describes your point of view on your income”. The response choices included “satisfied (4)”, “neither satisfied nor dissatisfied (3)”, “dissatisfied (2)”, “do not care (1)”, and “do not know (0)”. Responses of “do not care” and “do not know” were used to avoid missing values. The two created dummies included household income satisfaction (satisfied = 1, other responses = 0) and household income dissatisfaction (dissatisfied = 1, other responses = 0).
The self-rated health is measured by asking the respondents “All in all, how would you describe your state of health?” given the choice of the very good = 5; good = 4; neither = 3; poor = 2; very poor = 1. The dummy rating for good health was 1 if the respondents described their health status as “very good” or “good” and 0 for other responses. The dummy rating for poor health was 1 for “poor” or “very poor” responses and 0 for other responses.
The cross-country independent variables of national health expenditure (%) and age of older than 65 years (%) were constant values for each country. The national health expenditure is expressed as a percentage of the GDP, and population data were provided as a percentage of the national population. As government health expenditures come from tax revenue, current health spending as a percentage of the GDP was adopted as the interested independent variable. The population over 65 years of age as a percentage of the national population is derived from the World Bank’s (2019) study of aging populations.
Estimation StrategyWe used a logistic regression model to investigate the relationships between healthcare evaluation, inequality, the aging population, and healthcare affordability. The seven categories of binary dependent variables used included medical care systems or services ((1) importance, (2) satisfaction, (3) dissatisfaction), self-rated health ((4) good or (5) poor) and household income satisfaction ((6) satisfaction or (7) dissatisfaction). Logistic regression or probit regression is appropriate for binary dependent variables [35,36]. In this study, logistic regression analysis was adopted (Hijc = In (pijc 1 - pijc)), the pijc presents the probability that Hijc= 1. See equation (1):

where j denotes indices of seven categories of binary dependent variables; i refers to individuals in country C; and K denotes the national health expenditure (as a percentage of the GDP), which is shared by individuals within the given country C . X denotes a set of exogenous demographic and economic variables, which are introduced in section 2.2 (Variable Setting) on variables. D is the country dummy, which is expected to control for country-level heterogeneity; α is a constant term; and θ, β and δ are the estimated coefficients.
It is thought that public medical care expenditure improves public health and balance inequality. However, if nations experience hardship in the public medical care system, the national health expenditure reduces people’s satisfaction and increases dissatisfaction with the medical care system. Moreover, it increases the likelihood of household income dissatisfaction and reduces income satisfaction. Therefore, we identify the hardship regarding the affordability of medical care system if the estimated parameter θ for satisfaction of medical care is negative and evaluated with dissatisfaction is positive and for importance is negative values and statistically significant. Moreover, θ is negative for household income satisfaction and positive for household income dissatisfaction.
Equation (2) expresses the relationship between the medical care system and population aging.

where M denotes population aging as the percentage of people older than 65 years in the national population; a is a constant term; and b,f,d, and g are the estimated coefficients.
We hypothesized that national health expenditure positively affected well-being, which would improve the respondents’ subjective assessment of medical care systems or services and reduce health-related and financial inequalities. Accordingly, the negative values for the expected coefficients fj represented the dissatisfactory responses to such systems or services (“dissatisfied”), self-rated health (“poor”) and household income (“dissatisfied”). Conversely, positive values for j represented the responses to such systems or services (“important”), medical care (“satisfied”), and household income (“satisfied”).
We also hypothesized that population aging and national health expenditure would have the opposite effect on subjective well-being—the increasing age of the population in a nation negatively affects respondents’ evaluations of medical care systems or services, as well as negatively affects health-related and financial inequalities. Therefore, the burden of health affordability is considered severe. In this scenario, the coefficients of national health expenditure (fj and dj) represent the opposite ratings.
Pertinent statistics are presented in Table 1. Regarding the medical system services evaluation, 29% of respondents indicated their satisfaction, 29% of respondents showed their dissatisfaction, and 43% believed that evaluating the medical system was important. For perceived income satisfaction, 29% of households were satisfied, and 27% of households were dissatisfied with their household incomes. The average national health expenditure as a percentage of the GDP was 8.22%, and the population over 65 years of age as a percentage of the national population was 14.1%. Figure 1 displays the multinational percentages of dissatisfaction with the medical care system or services, as well as the relative efficiency compared with that of the United States. The United States and Japan present lower medical care system dissatisfaction compared to national health expenditures. Developed nations tend to have better medical care system operation performance than developing nations.
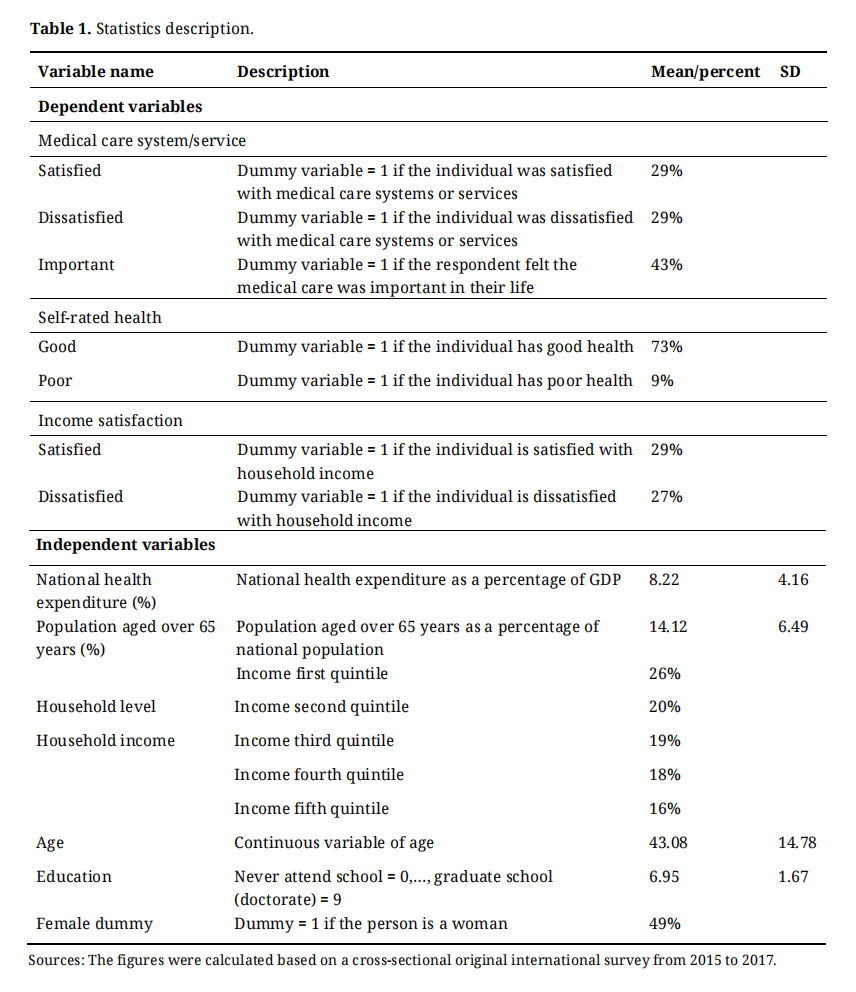 Table 1. Statistics description.
Table 1. Statistics description.
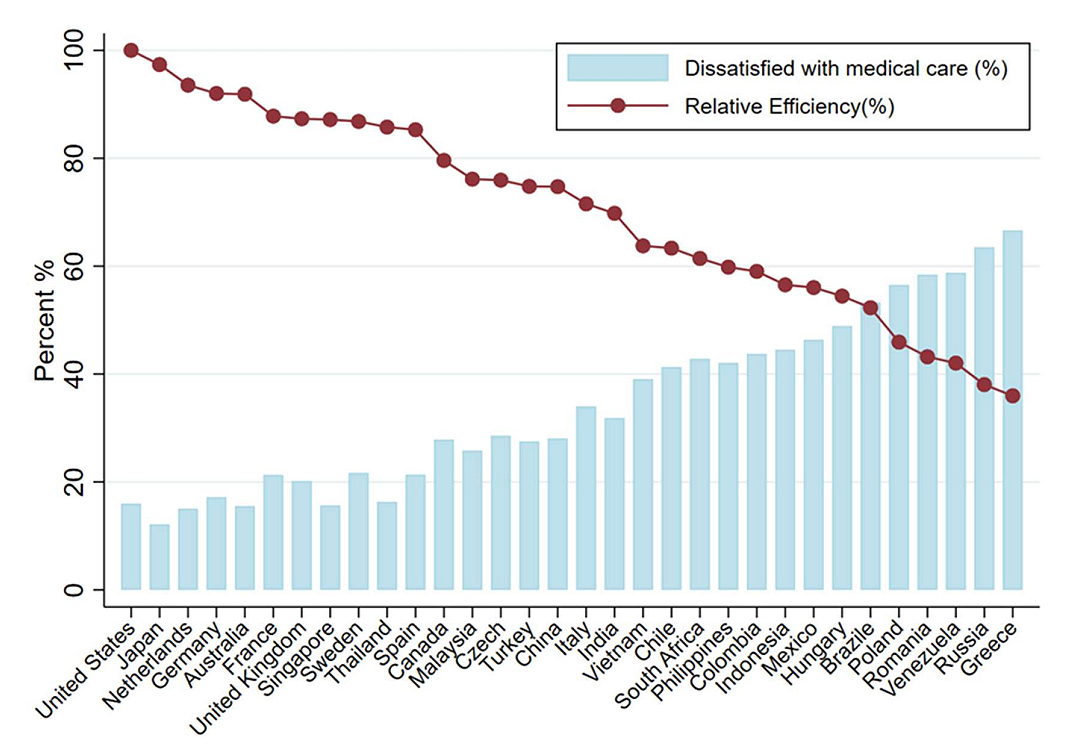 Figure 1. Multinational percentage of dissatisfaction with medical care systems/services. Note: Relative efficiency denotes the ratio of national public health expenditure and the dissatisfaction felt with public medical care; the United States as the comparator value is normalised as 100.
Figure 1. Multinational percentage of dissatisfaction with medical care systems/services. Note: Relative efficiency denotes the ratio of national public health expenditure and the dissatisfaction felt with public medical care; the United States as the comparator value is normalised as 100.
Table 2 displays the estimated marginal effects of the covariables from the logistic regression (see equation (1)), which were obtained using pooled samples from 37 nations. The regression included the subjective evaluation of medical care systems or services (important, satisfied, or dissatisfied), self-rated health (good or poor), and income (satisfied or dissatisfied) and considered them related to the national health expenditure of GDP (%), with other variables being used as controls.
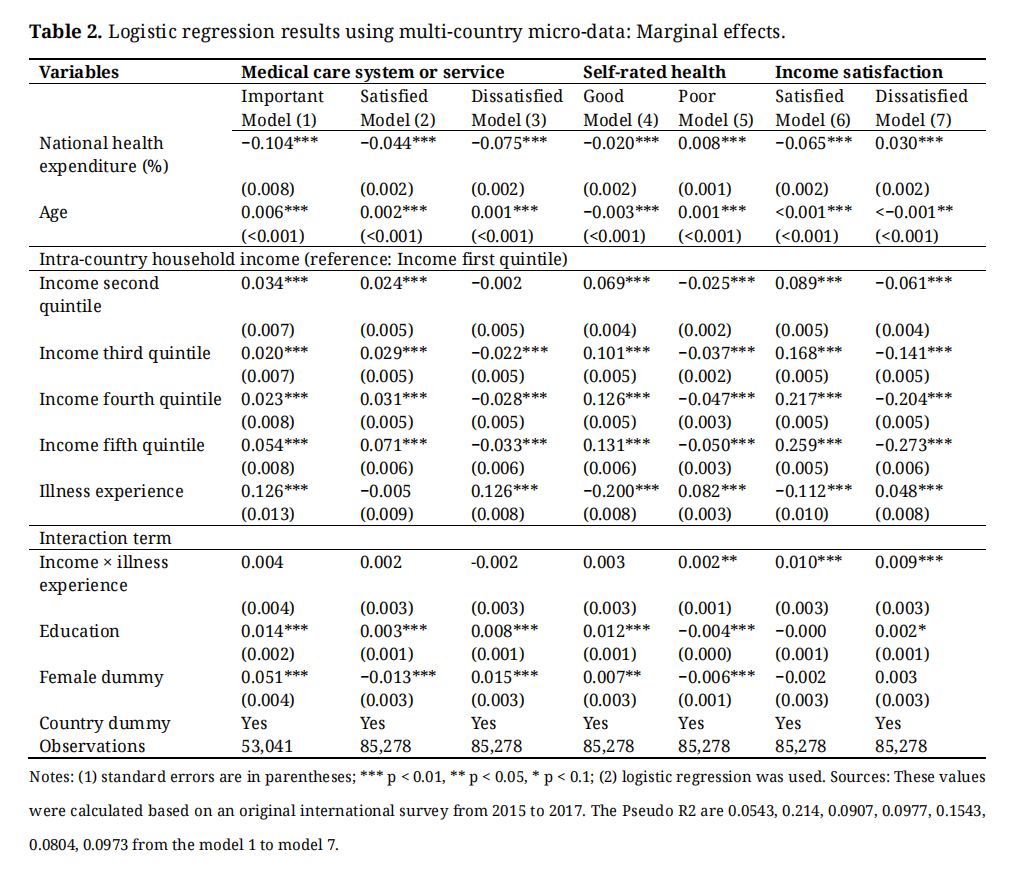 Table 2. Logistic regression results using multi-country micro-data: Marginal effects.
Table 2. Logistic regression results using multi-country micro-data: Marginal effects.
The coefficient of national health expenditure was −0.104, and it was statistically significant at the 1% level (Model 1). This result suggests that when national health expenditure increases by 1% (as a percentage of GDP), the percentage of individuals who consider using medical care systems or services decreases by 10.4%. The results from Models 2 and 3 revealed that a 1% increase in national health expenditure reduced satisfaction with these systems or services by 4.4%, as well as reduced dissatisfaction with the systems or services by 7.5%. These results indicate that increasing the national health expenditure of GDP reduces the dissatisfaction felt with medical care systems or services; however, the results also demonstrate that fewer individuals feel satisfied with medical care, and the cross-country effect is great.
Regarding the household income satisfaction assessments (Models 6 and 7), the coefficients of national health expenditure were −0.065 and 0.030, and they were statistically significant at the 1% level. These results suggest that increasing national health expenditure by 1% decreases individual satisfaction with income by 6.5%, as well as increases dissatisfaction with household income by 3%. The results are consistent with the previous studies [21–23]. However, for self-rated health assessments (Models 4 and 5), the coefficients of the national health expenditure were –0.020 and 0.008, and they were statistically significant at the 1% level. These results demonstrated that increasing national health expenditure decreased individuals’ reports of good health and increased their reports of poor health status. Overall, the results from Models 1 to 7 indicate that national health expenditure appears to have limited positive effects on the subjective well-being of individuals. Table 2 outlines the effects of national health expenditure on subjective well-being, without considering population aging.
Table 3 presents the estimated marginal effects of the key independent variables from the logistic regression (see equation (2)), in which pooled samples from 37 nations were used. The independent variables of interest included the national health expenditure of GDP (%) and the population older than 65 years (expressed as a percentage of the total population). When this study’s analysis concentrated on the effect of national health expenditure, population aging had to be controlled by including the population older than 65 years.
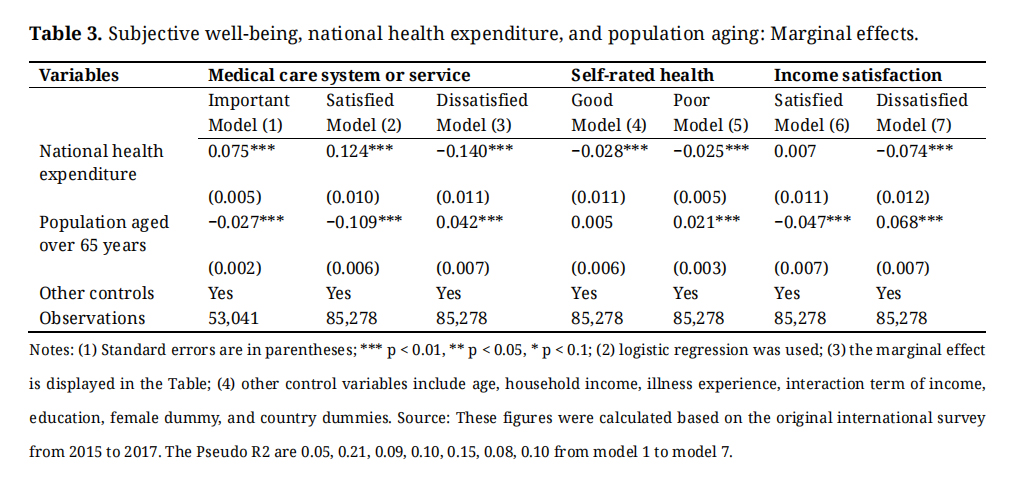 Table 3. Subjective well-being, national health expenditure, and population aging: Marginal effects.
Table 3. Subjective well-being, national health expenditure, and population aging: Marginal effects.
When population aging was added as an independent variable, the coefficients of national health expenditure changed significantly. The coefficients of national health expenditure for “important”, “satisfied”, and “dissatisfied” ratings regarding the medical care systems or services were 0.075, 0.124, and −0.140, respectively, and they were statistically significant at the 1% level. The results indicated that a 1% increase in national health expenditure would result in 7.5% and 12.4% more individuals who felt the such systems or services are “important” and who felt “satisfied”, respectively. The results are consistent with the previous studies [3–5]. Moreover, such an increase would result in 14% fewer individuals feeling dissatisfied with medical care. However, the coefficients of national health expenditure regarding household income dissatisfaction were negative (Model 7); further, they were positive values for income satisfaction (Model 6). These results reveal that increasing national health expenditure decreases national financial inequality. Similar trends were found regarding self-rated health. In brief, when the population aging effect was removed, the national health expenditure decreased national financial and health-related inequalities and improved individual response to medical care systems or services.
The opposite effect was also observed in the analysis of national health expenditure and population aging in terms of medical care evaluation, self-rated health, and household income satisfaction. For example, regarding medical care systems or services, the coefficients of the population aged older than 65 years were −0.027, −10.9, and 0.042, and they were statistically significant at the 1% level. These results indicate that the aging population significantly worsened individuals’ evaluations of such systems or services. Similarly, the coefficients for the population aged older than 65 years were −0.047 and 0.068, and they were also statistically significant at the 1% level. These results reveal that the aging population correlates with worsened individual satisfaction with household income.
The main effects of health expenditure in this study included decreased medical care dissatisfaction and improved satisfaction, as well as non-improved national self-rated health status. When the coefficients of national health expenditure were compared with those of medical care satisfaction or dissatisfaction and self-rated health (“poor”), the coefficients of self-rated health were observed to be smaller than the corresponding coefficients of medical care satisfaction or dissatisfaction. This result might be due to the long-term care burden on national health expenditures.
The policy implications based on the results derived in this study are as follows. The first main result of this study and policy implication relates to the national health expenditure’s complex effects on individuals’ medical care system evaluation, income satisfaction, and self-rated health. The increase in health expenditure decreased the respondents’ self-evaluated satisfaction of medical care or services and increased their probability of feeling dissatisfied with the medical care system. The increasing national health expenditure also prompted them to evaluate the importance of the medical care systems or services in connection with their life satisfaction, to a lesser extent. Regarding income satisfaction, when public health expenditure increased, respondents’ satisfaction with their family income decreased. National health expenditure reduced the likelihood of evaluating the health status and increased the number of adults who experienced poor health.
The second main result of this study and policy implication is that increasing national health expenditure complexly affects peoples’ subjective reports of well-being. The effects of an aging population play an important role in increasing national medical care systems or services experience, which challenges national health affordability. When the population aging effect is removed, individuals positively evaluate increasing national health expenditure. Results show that individuals are likely satisfied with medical care systems or services and income; they likely consider them important and believe that they improve the population’s poor health status and hence are less likely to be dissatisfied with the systems or services.
This study, which investigated the relationship between national health expenditures and individuals’ self-rated satisfaction with health, income, and the medical care system, has several limitations. First, the data were mainly obtained via the internet; thus, the collected sample included a disproportionate number of well-educated individuals and wealthy households. Thus, it is not representative of actual demographics. To address this issue, future studies should use more comprehensive data to analyze the relationship between national health expenditures and citizens’ evaluations. Second, this study used logit and probit models for analysis to indicate the association between national health expenditures and citizens’ well-being. In future studies, these models should estimate the casual relationship to obtain an in-depth understanding of issues concerning medical care system affordability.
Along with the economic development, the couples tend to marriage later and have fewer children in the recent decades and as a consequence the population aging issue become severe. The medical care burden become severe when the ratio of the old-aged population aging is greater than ever before. To improve the middle- and old-aged individuals’ health status. This study investigated survey participants’ opinions regarding healthcare, and it measured the subjective inequality, population age, and sustainability of affordable health in various countries with aging populations. This large-scale, original survey involved more than 100,000 respondents from 37 nations who participated online or in face-to-face sessions. Logistic regression models and ordered logistic regression models were used to analyze the changes in health affordability based on individual opinions and social activities around medical care services.
For the original cross-sectional internet survey through a third-party company (Nikkei Research Company) between 2015 and 2017, the study design was approved by the appropriate legal and ethics review board of Kyushu University. The data were collected with informed consent from participants, according to legal and ethical guidelines. All the methods were in accordance with ethical guidelines and approved by the ethical committee of Kyushu University.
The following supplementary materials are available online at https://doi.org/10.20900/jsr.20140011. Supplementary Table S1: Survey information.
This data are not publicly available due to data affiliation relationships.
The author declares that there is no conflicts of interest.
This Research is supported by Takahashi Industrial and Economic Research Foundation, Grant number J220000023. This research is supported by JSPS KAKENHI (Grant Number Grant Number 23K17082). This research was funded by Support for research activities through the Women’s Activity Transformation Program 2023 Iwate University.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
Piao X. Multinational Medical Care Evaluation Concerning Aging Populations. J Sustain Res. 2024;6(2):e240011. https://doi.org/10.20900/jsr20240011

Copyright © 2023 Hapres Co., Ltd. Privacy Policy | Terms and Conditions




